- Projects

01.12.2021 by Philippe Bechtold, Philipp Wagner, Salome Hosch, Denise Siegrist, Amalia Ruiz-Serrano, Michele Gregorini, Maxmillian Mpina, Florentino Abaga Ondó, Justino Obama, Mitoha Ondo’o Ayekaba, Olivier Engler, Wendelin J. Stark, Claudia A. Daubenberger and Tobias Schindler*
Abstract
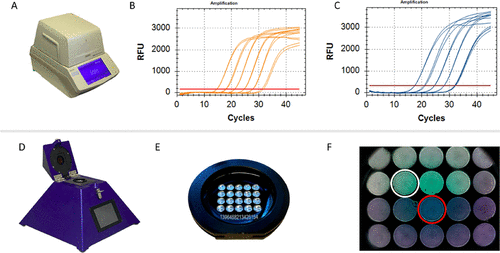
The need for tools that facilitate rapid detection and continuous monitoring of SARS-CoV-2 variants of concern (VOCs) is greater than ever, as these variants are more transmissible and therefore increase the pressure of COVID-19 on healthcare systems. To address this demand, we aimed at developing and evaluating a robust and fast diagnostic approach for the identification of SARS-CoV-2 VOC-associated spike gene mutations. Our diagnostic assays detect the E484K and N501Y single-nucleotide polymorphisms (SNPs) as well as a spike gene deletion (HV69/70) and can be run on standard laboratory equipment or on the portable rapid diagnostic technology platform peakPCR. The assays achieved excellent diagnostic performance when tested with RNA extracted from culture-derived SARS-CoV-2 VOC lineages and clinical samples collected in Equatorial Guinea, Central-West Africa. Simplicity of usage and the relatively low cost are advantages that make our approach well suitable for decentralized and rapid testing, especially in resource-limited settings.
Introduction
Full publication:
diaxxoPod (RUO)

Our in-vitro diagnostic test cartridge based on rapid Polymerase Chain Reaction (PCR) amplification technology. This cartridge can reliably detect and distinguish the mutants from UK (20I/501Y.V1, B.1.1.7 – VOC-202012/01) as well as the South African mutation (B.1.351 lineage).
The test cartridge is aimed to improve the public health situation by rapidly enabling the detection of variants of concern. The cartridge is designed for qualitative detection of variants of interest of the SARS-CoV-2 Viral RNA in saliva samples and it works in conjuction with diaxxoPCR.
The test cartridges are sold with all the necessary reagents pre-loaded in the reaction wells. The use of the test cartridges is therefore extremely simple:
diaxxoPod

The test cartridges are sold with all the necessary reagents pre-loaded in the reaction wells. The use of the test cartridges is therefore extremely simple:
We use cookies on our website to give you the most relevant experience by remembering your preferences and repeat visits. By clicking “Accept”, you consent to the use of ALL the cookies.